Ackerson, L. K. and S. V. Subramanian (2008). "Domestic Violence and Chronic Malnutrition among Women and Children in India." American Journal of Epidemiology.
Ammaniti, M., A. M. Ambruzzi, et al. (2004). "Malnutrition and Dysfunctional Mother-Child Feeding Interactions: Clinical Assessment and Research Implications." Journal of the American College of Nutrition 23(3): 259–271.
Baker-Henningham, H., C. Powell, et al. (2005). "The effect of early stimulation on maternal depression: a cluster randomised controlled trial." Arch Dis Child 90: 1230–1234.
Be'gin, F., J.-P. Habicht, et al. (1997). "The Deterioration in Children's Nutritional Status in Rural Chad: The Effect of Mothers' Influence on Feeding." Am J Public Health 87: 1356-1359.
Bégin, F., J. E. A. Frongillo, et al. (1999). "Caregiver Behaviors and Resources Influence Child Height-for-Age in Rural Chad." Journal of Nutrition (JN) 129: 680-686.
Black, R. E., L. H. Allen, et al. (2008). "Maternal and child undernutrition: global and regional exposures and health consequences." Lancet 371: 243–260.
Casapı´a, M., S. A. Joseph, et al. (2007). "Parasite and maternal risk factors for malnutrition in preschool-age children in Belen, Peru using the new WHO Child Growth Standards." British Journal of Nutrition 98: 1259–1266.
Delpeuch, F., P. Traissac, et al. (1999). "Economic crisis and malnutrition: socioeconomic determinants of anthropometric status of preschool children and their mothers in an African urban area." Public Health Nutrition 3(1): 39-47.
El-Sayed, N., A. G. Mohamed, et al. (2001). "Malnutrition among Pre-school Children in Alexandria, Egypt." J Health Popul Nutr 19(4): 275-280.
Engle, P. L., P. Menon, et al. (1999). "Care and Nutrition: Concepts and Measurement." World Development 27(8): 1309-1337.
Galloway, A. T., L. M. Fiorito, et al. (2006). "‘Finish your soup’." Appetite 46(3): 318–323.
Golden, M. H., M. P. Samuels, et al. (2003). "How to distinguish between neglect and deprivational abuse." Archives of Disease in Childhood 88: 105-107.
Gragnolati, M., M. Shekar, et al. (2005). India’s Undernourished Children: A Call for Reform and Action. Washington, DC USA, Health, Nutrition, and Population Family - World Bank.
Harpham, T., S. Huttly, et al. (2005). "Maternal mental health and child nutritional status in four developing countries." J Epidemiol Community Health 59: 1060–1064.
Hassan, H., W. Moussa, et al. (2006). Assessment of dietary changes and their health implications in countries facing the double burden of malnutrition: Egypt, 1980 to 2005. The double burden of malnutrition Case studies from six
Tuesday, March 30, 2010
Conclusion
Undernutrition among under five years is still a major public health issue in Cameroon regardless the efforts registered during the past decades. It is the result of a combination of well known socioeconomic and biological factors, in association with psychological factors that are under estimated and contextual factors.
Rural areas are more at risk than urban zones and poverty is a grounded matrix with complex infractions between a wide range of factors including; child’s characteristics, mother’s features, household and family attributes and psychological determinants.
Thus the national program implementation is likely to be succesfull if this considerations are well integrated at the central level, at the operational level with a strong commitment of all the stakeholders; it is suitable to incorporate psychological approach combine with socio economical activities to improve efficiency of strategies against undernutrition
Operational research should be part of the interventions in order to timely trace significant changes for capitalisation of good practices and improvment of less satisfactory ones.
Further studies should carry out to better highlight the psychological determinants as well as others new vision about under five year undernutrition; aiming to buld a comprehensive Infant and child survival interventions.
Rural areas are more at risk than urban zones and poverty is a grounded matrix with complex infractions between a wide range of factors including; child’s characteristics, mother’s features, household and family attributes and psychological determinants.
Thus the national program implementation is likely to be succesfull if this considerations are well integrated at the central level, at the operational level with a strong commitment of all the stakeholders; it is suitable to incorporate psychological approach combine with socio economical activities to improve efficiency of strategies against undernutrition
Operational research should be part of the interventions in order to timely trace significant changes for capitalisation of good practices and improvment of less satisfactory ones.
Further studies should carry out to better highlight the psychological determinants as well as others new vision about under five year undernutrition; aiming to buld a comprehensive Infant and child survival interventions.
A Sample of Parteners
Local NGOs active in health sector
African Program for Onchocerciasis Control (APOC)
Canadian International Development Agency (CIDA)
Lions Club International Foundation (LCIF) and Sight First Program
Population Services International (known as ACMS in Cameroon)
Red Cross
Rotary International
United States Agency for International Development (USAID)
Medecins Sans Frontière (MSF)
UNICEF

UNICEF Goodwill Ambassador Ms. Farrow visited a UNICEF-supported nutrition centre in Bazzama village, eastern Cameroon
Plan Cameroon

Plan Cameroon is active in more than 14 health districts
HKI

Helen Keller International during a community based deworming (onchocerchiais)
African Program for Onchocerciasis Control (APOC)
Canadian International Development Agency (CIDA)
Lions Club International Foundation (LCIF) and Sight First Program
Population Services International (known as ACMS in Cameroon)
Red Cross
Rotary International
United States Agency for International Development (USAID)
Medecins Sans Frontière (MSF)
UNICEF
UNICEF Goodwill Ambassador Ms. Farrow visited a UNICEF-supported nutrition centre in Bazzama village, eastern Cameroon
Plan Cameroon
Plan Cameroon is active in more than 14 health districts
HKI
Helen Keller International during a community based deworming (onchocerchiais)
Operational level
The 178 District Health Services whose mission is to implement national health policy and interventions in their Health District catchement area, constitute the operational level of the"ENA Appraoach". They offer health care and services according to the national health policy describe in the Sectorial Health strategy 2001 - 2015.
As such,they plan all the activities related to the health sector. They organize, implement and follow up “fight against disease” programs. they organize, implement and follow up health promotion programs. They organize the supervision of the activities of the district health service, public and private health facilities, meanwhile and the reference counter reference system. They organize, implement and follow up care in Hospitals. On a periodic base, They monitor and report the activities of all actors in the health sector of the District. They ensure epidemiological awareness in the Health District. They follow up the command and the management of pharmaceutical products and medical devices by the Health facilities. They execute and follow up investment projects. They collect, analyze and use health data. They ensure maintenance of biomedical equipments. They manage human resources. They manage vehicles. They mobilize all actors and resources for Health issues.
Overall, the health District services are key component of the hole approach and their leadership, competences, planning and management skills, coordination inovative mobilisation capacities, as well as their expertise is a must for onership of implementation actions and sustanability of achievments.
The pathway for national program

The sites of activities

Monday, March 29, 2010
National Program "Essential Nutrition Actions"
Cameroon's Ministry of Public Health is implementing a national program with the following team:
Okala Georges, Ndongmo N. Augustin, Toumamiko Barthelémy, Amadou Boukari, Nankap Martin
"ESSENTIAL NUTRITION ACTIONS" (ENA) is an operational oriented program integrating mother and child nutritional status and national environment, sumarized in the following framework.
Its specificities is:
An Integrated Program for:
Infant and young child nutrition
Mother nutrition
Micronutrient completion.
As such the following issues should be adressed:
Promotion of optimal breasfeeding
- Initiate breastfeeding within 30 minutes after birth
- Breastfeed exclusively up to 6 months
- Breastfeeding on demand, day and night, at least 10 times
- Practicing latch and position correct
- Empty one breast before switching to anotherPromotion of complementary feeding
Promotion of adequate complementary feedind
- Start complementary feeding at 6 months
- Breastfeeding until 24 months and beyond
- Increase the number of meals and variety of food with age
- Increase the density and volume with age
- Practice active feeding
- Practice good hygiene (water, food, clean hands)
- Use fortified complementary foods
Provide nutrition care of sick and malnourish children
0 to 6 months:
- Increase frequency of breastfeeding during and after illness
- Giving zinc and vitamin A, according to the national protocol (IMCI)
- Rehydrate orally, as needed
Over 6 months:
- Increase frequency of breastfeeding during and after illness and
- Increasing the supply during and after illness
- Give an extra meal each day for 2 weeks
- Giving zinc and vitamin A, according to the national protocol (IMCI)
- Rehydrate orally, as needed
- Caring for severely malnourished children according to national protocolStart complementary feeding at 6 months
Promotion of mothers nutrition
During pregnancy and lactation:
- Increasing dietary intake: (1 meal per day during pregnancy, 2 during breastfeeding)
- Supplementing iron-folic acid (6 months)
- Preventing and treating malaria
- Deworming during pregnancy
- Take Vitamin A post within 8 weeks after childbirth
Fight aigainst vitamine A deficiencies
- Promoting breastfeeding as a source of Vitamin A
- Promote the consumption of rich foods and foods rich in Vit A (industrial or household)
- Supplementing women after childbirth
- Supplementing the children twice a yearFight aigainst anemia
Fight aigainst anemia
- Supplementing iron-folic acid for women
- Deworming during pregnancy and children 2 times per year
- Preventing and treating malaria
- Promote the consumption of rich foods and foods fortified with iron (industrial or household)
- Delaying the umbilical cord ligation (after 2 minutes)Fight aigainst iodine deficiency disorders
Fight aigainst iodine deficiency disorders
- Promote consumption of iodized salt by all families
Sunday, March 28, 2010
Signs & Management
Clinical signs
Main characteristic: Weight for age, height for age, weight for height or BMI are below -2 z score.
Secondary characteristic:
- Oedema
- Skin nail and hair changes
- Enlargement or tenderness of liver, jaundice
- Abdominal distension, bowel sounds, “abdominal splash” (a splashing sound in the abdomen)
- Severe pallor
- Signs of circulatory collapse: cold hands and feet, weak radial pulse, diminished consciousness
- Temperature: hypothermia or fever
- Thirst
- other signs of infections eventually
Biological signs
They are specific to associated diseases that are usually associated
Treatment
Treatment in health facilities for severe cases
Balanced diet and treatment of secondary diseases for acute and non severe cases
Nutritional rehabilitation for the child, empowerment of families and comunities in low income settings, psychological interventions for families in chronic and endemic settings.
Conflicts and disaster management for basic causes.
Data 1980 - 2006 WHO Data Base
Undernutrition for under five has been without improvment from 1998 to 2004. as such it remains a public heath issue for the country and a challenge for different strategies.
The Cameroon government is taking the issue siriously and has adressed target by the year 2015 in the Health strategic plan 2001 to 2015.
The institution in charge is the "Ministry of Public Health, Direction of Health Promotion, Nutrition Division. This service coordinates the intervertions at national level and the diversify international contributors ( WHO, UNICEF, MSF, Plan Cameroon, GTZ, LNGOs) as well as private initiatives.
The strategies of Ministry of Public Health are implemented at the District level (178) uner the coordination of regional Delegates (10).
These straegies combine clinical an community based interventions.
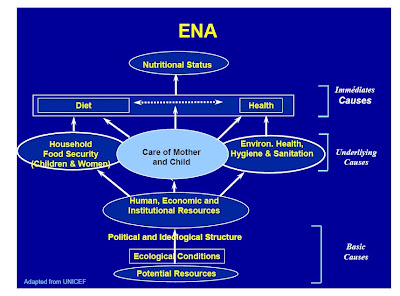
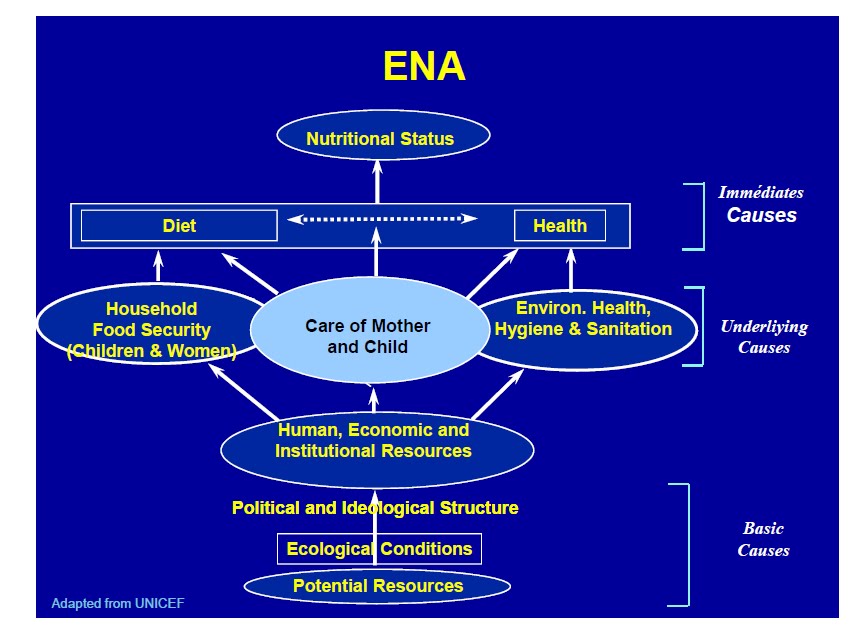
Causes
The Immediat cause of undernurition is an inbalanced diet;
The underliying causes are:
Inapproppriate/insufficient food supply, poor breastfeeding and winning management, culture and religious food customs.
There is also a wide range of contributing factors in the literature as described below:
The rural areas are the most affected by under nutrition among under five years. This could be linked to low diversity of food sources in these remote areas compare to urban cities, as well as poverty.
In many studies children characteristics as gender, birth weight, age, illnesses, child order among others in the family and child spacing, are potential contributing factors to the issue. Researchers have different views related to the gender more prone to undernutrition. This can be explained by competition.
Another common findings in many studies is the parents education in general and mostly mother education strongly related to undernutrition prevalence this can be explained by the fact that educated women in contrary of non educated ones, are likely to seek for help and care in case of difficulty, they also are incline to adopt new medical advices for child health improvement. The mother’s education contributes to mother’s empowerment and women are child centered in expenditures, thus likely to acquire the child’s needs.
Maternal health status is not the least in this bundle of predictive factors for under five years under nutrition, especially in relation with early unset childhood undernutrition. Low mother body mass index, low height and perinatal depression have been described to increase risk of undernutrition. This could be also explained by reduce or lack appropriate health-seeking behavior in depressed mothers, and also a reduction in child needs awareness, another mechanism is by the impairment of mother child relationship. Interaction between mother and child including breast feeding pactice, is another predictor of child undernutrition often ignored. Reduce attention or over pressure on the child during feeding have negative influences on appropriate food intake of the child.
The situation is of concern with basic causes as the refugees sitation resulting from civil crisis in neighbouring countries; namely Tchad and Centrafican Republic.
Introduction
Malnutrition
Defining by World Health Organization, is as "the cellular imbalance between supply of nutrients and energy and the body's demand for them to ensure growth, maintenance, and specific functions”(WHO Onis M. et al. 1993)This encompases, protein-calorie malnutrition (undernutrition and overnutrition) as well as micronutrient insufficiencies (iodine, iron, copper, thiamine, riboflavin, ascorbic acid, retinol, tocopherol, cobalamin, vitamin A, vitamin K, selenium, zinc, nitrogen, carbon skeleton of essential amino acids (Lysine, Threonin), sodium, potassium, phosphorus, sulphur, magnesium, manganese, vitamin D).
This paper confined in "under five years undernutrition" in cameroon; this target constitute a priority in public health interventions with regards to their vulnerability to malnutrition. Another reason is that stigma of child malnutrition (including undernutrition) is likely to impact adulthood.
Sample indicator
 Length for Age
Length for Age
Developing countries estimates of prevalence of Underweight Children in 1980 - 2005

Stunting in preschool children 1980 - 2005
Proportinal mortality in children younger than five years old in developing countries
 Proportional distribution of Health threat in developing countries
Proportional distribution of Health threat in developing countries
Defining by World Health Organization, is as "the cellular imbalance between supply of nutrients and energy and the body's demand for them to ensure growth, maintenance, and specific functions”(WHO Onis M. et al. 1993)This encompases, protein-calorie malnutrition (undernutrition and overnutrition) as well as micronutrient insufficiencies (iodine, iron, copper, thiamine, riboflavin, ascorbic acid, retinol, tocopherol, cobalamin, vitamin A, vitamin K, selenium, zinc, nitrogen, carbon skeleton of essential amino acids (Lysine, Threonin), sodium, potassium, phosphorus, sulphur, magnesium, manganese, vitamin D).
This paper confined in "under five years undernutrition" in cameroon; this target constitute a priority in public health interventions with regards to their vulnerability to malnutrition. Another reason is that stigma of child malnutrition (including undernutrition) is likely to impact adulthood.
Sample indicator
Developing countries estimates of prevalence of Underweight Children in 1980 - 2005
Stunting in preschool children 1980 - 2005
Proportinal mortality in children younger than five years old in developing countries
Saturday, March 20, 2010
The country
 CAMEROON
CAMEROONComplete Name: Republic of Cameroon
Native Name: Cameroun, Cameroon
ISO-Code: CMR
Capital: Yaoundé
Population 2007: 18,674,600
http://images.google.com/images?q=cameroon&hl=en&sa=N&tbs=isch:1
Cameroon History
After the 2nd world war, Cameroon territory has been under the mandate of British and French Goverments.
The former French Cameroon and part of British Cameroon merged in 1961 after a national referendum to form the present country.
The leadear is the President Paul BIYA
http://upload.wikimedia.org/wikipedia/commons/6/67/Paul_Biya_at_US_Embassy_2006.JPG
and the Prime Minister chief of government is Philemon YANG since july 2009
http://www.camnet.cm/uploads/news/id112/yang.jpg
You will find in the following link an overview of the country
The country is divided into ten regions headed by Governors of regions
namely
1) Adamaoua region, 2) Center region who chairs the headquaters of institutions in Yaoundé, 3) East region, 4) Extreme North region, 5) Littoral region, 6) North region, 7) North West region, 8) West region, 9) Sud region, and 10) south West region.
Cities and Populations
http://www.citypopulation.de/Cameroon.html#Land
Subscribe to:
Posts (Atom)
{kind=link}
{kind=link}
{kind=link}
{kind=link}